Paget’s Disease

General Information
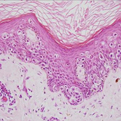
As depicted in Jane Austen’s Pride and Prejudice reality may not be reflected in an initial impression or appearance. So to, cutaneous Paget’s disease maybe an important harbinger of an underlying visceral malignancy. The most important forms of Paget’s disease entail a genital or extra-mammary form imbued a tenuous association with underlying genitourinary or gastrointestinal adenocarcinoma and a mammary form of the disease which connotes an inevitable association with underlying breast adenocarcinoma. Both forms represent the intra-epithelial proliferation of glandular-derived malignant cells. These cells derive from the adnexal or adnexal-like apocrine or sebaceous glands of their respective anatomic structures. The pathogenic mechanisms or etiology of these diseases remains unknown, as does the exact pathogenic relationship that these tumors potentially possess with their respective underlying malignancies. The clinical presentation involves a scaly patch of the breast nipple or an erythematous patch of the genitalia. The pathology is typically configured as a confluent and randomly scattered spread of abnormal polygonal-shaped clear cells throughout the epithelium. The confluent foci tend to be seen in basilar portions of the epithelium with some tendency of these cells to coalesce forming glandular foci with central lumina seen. The cells themselves possess ample amounts of foamy-to-clear cytoplasm with occasional vacuoles. The nuclei are enlarged and possess prominent central nucleoli. These cells sometimes referred to as Paget cells, are typically carcinoembryonic antigen (CEA), cytokeratin-7, epithelial membrane antigen positive and cytokeratin-20, high molecular weight keratin, S-100 and leukocyte common antigen (LCA) negative on immunohistochemical staining. The latter stains are important to examine as the most important entities that can masquerade as Paget’s disease and entail the pagetoid scatter of atypical intraepidermal cells include CK-20 merkel cells, high molecular weight keratin squamous cell carcinoma cells, S-100 melanoma cells, and LCA lymphoma cells. The prognosis of mammary Pagets disease remains guarded and given its inviolate association with underlying breast adenocarcinoma, is treated with local surgery often entailing mastectomy with adjuvant radiotherapy and chemotherapy. Genital forms of the disease portend a significantly better prognosis with approximately 20% associated with underlying cervical, bladder, prostate or colorectal adenocarcinoma. The cutaneous expression of the disease even among patients with demonstrated visceral involvement, can be successfully treated with frozen section aided excisional or Mohs micrographic surgery.
Epidemiology
Uncommon, elderly, mammary and extra-mammary
Etiology
Unknown
Pathogenesis
Single and nested clear cells throughout the epithelium, CEA+, CK-7+, EMA+
Clinical
Scaly or erythematous patch areola or genitalia
Histology
Supportive for mammary, excision with genitourinary/gastrointential w/u for extra-mammary.
Bibliography
1. Jones R, Austin C, Ackerman A. Extramammary Pagets Disease: A critical reexamination. Am J Dermatopathol 1979; 1: 101. 2. Lee S, Roth L, Ehrlich C, et al. Extramammary Pagets Disease of the vulva. A clinicopathologic study of 13 cases. Cancer 1977; 39:2540. 3. Chanda J. Extramammary Pagets Disease: Prognosis and relationship to internal malignancy. JAAD 1985; 13: 1009.
Download PDF
![]() Paget’s Disease
Paget’s Disease