Basal Cell Carcinoma

General Information
Basal Cell Carcinoma (BCC) is the most common cutaneous carcinoma with an annual U.S. incidence of approximately 900,000 cases, outnumbering the next most prevalent carcinoma (squamous cell carcinoma) by a factor of four and melanoma by a factor of 20. Common to the aforementioned neoplasms, the etiology of BCC is most closely related to excessive ultraviolet exposure and accordingly, is most commonly diagnosed in the elderly, on the exposed cutaneous surfaces and in sunny geographic locales. Exceptions to this rule are rare yet can be observed in certain genetic syndromes that may predispose to multiple BCC’s occurring in exceptional anatomic locations and age ranges. These syndromes include xeroderma pigmentosa, the Basex and Basal Cell Nevus syndromes. It is in the latter syndromes that the pathogenesis has been discerned and relates to the development of sporadic forms of this disease as well. The pathogenesis involves mutations in the human homologue of the Drosophila gene patched (PTCH1) where it functions as a tumor suppressor gene. Loss of this gene or its function along with acquired (ultraviolet-induced) defects in the p53 gene and the apoptosis-regulating gene BAX has also been implicated in the pathogenesis. Regardless of their underlying cause, these neoplasms may present in a variety of clinical guises depending upon the type or variant disclosed. These variants may be broadly sub-categorized on the basis of their respective biologic behaviors as indolent or aggressive. The indolent variants include the most common, nodular type responsible for 75% of cases and typically configured as slow-growing skin-toned papule with surface telangectases located on the face. The next most common indolent variant is the superficial type, typically presenting on the trunk or extremities as a slowly expanding erythematous and scaly patch. A rare variant known as the Pinkus type, typically presents as a slow-growing soft nodule on the trunk or proximal extremities. Finally, there is the keratotic variant which is considered indolent yet important to histologically distinguish from one of the more aggressive variants known as the basosquamous or metatypical variant. The aggressive variants include infiltrating, morpheaform, basosquamous and micronodular types. The infiltrating and morpheaform types similarly present as more rapidly expanding ill-defined erythematous indurated patches located on the face. The basosquamous variant typically presents as a rapidly growing often hyperkeratotic and ulcerated nodule on the face. The micronodular variant is capable of presenting in a variety of guises including non-descript truncal or extremity papules.
Epidemiology
900,000 a year U.S., incidence increasing 5% a year, Caucasians
Etiology
Ultraviolet exposure, irradiation, ulceration, burns, arsenic, coal-tar, genetics.
Pathogenesis
PTCH, p53, BAX gene mutations
Clinical
Nodular-facial telangectatic papule, superficial-scaly truncal patch, infiltrating/morpheaform-ill-defined erythematous indurated facial patches.
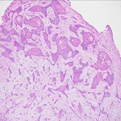
Histology
Nodular-large nodules with central necrosis, superficial-Multifocal superficial de-limited basaloid islands, pinkus-retiform extensions of anastomosing basaloid tumor, keratotic nodular saloid tumor with central mature keratinization, infiltrating-irregular thick and thin islands of deeply extending basaloid tumor, morpheaform –irregular uniformly thinned basaloid tumor coursing throughout dermis, basosquamous-composite tumor comprised of malignant squamous foci with basaloid foci, and micronodu
Bibliography
1. Miller D, Weinstock M. Non-melanoma skin cancer in the United Staes:incidence. JAAD, 30: 774-8, 1994. 2. Asterbaum M, Rothman A, Johnson R, et al. Identification of mutations in the human PTCH gene in sporadic basal cell carcinomas and in patients with the basal cell nevus syndrome. J Invest Dermatol 110: 885-8, 1998. 3. Weedon D, ed. Pathology of Basal cell Carcinoma In: Skin Pathology. Churchill Livingstone, London, 2002.
Download PDF
![]() Basal Cell Carcinoma
Basal Cell Carcinoma